A Review of Total Hip Arthroplasty, Hip Resurfacing and Minimally-Invasive Hip Surgery
Edited by Nick Hernandez, M.D., Assistant Professor, UW Orthopaedics & Hip & Knee
Did you know...?
- That modern total hip replacement was first performed in the early 1960s and the surgeon who pioneered the procedure was honored with knighthood by the Queen of England?
- That traditional total hip replacement--similar in many ways to the procedure performed over 40 years ago--is considered by many to be the most important operation developed in the 20th century in terms of the amount of human suffering it has relieved?
- That a wide variety of materials have been used in the manufacture and insertion of hip replacements--including Teflon (tm)--but that only a few seem to work very well?
- That in hip replacement as in so many other areas of life newer is not always better...
Total hip replacement (THR) is a surgical procedure that relieves pain from most kinds of hip arthritis improving the quality of life for the large majority of patients who undergo the operation.
Patients commonly undergo THR after non-operative treatments (such as activity modifications medications for pain or inflammation or use of a cane) have failed to provide relief from arthritis symptoms. Most scientific studies that have followed patients for more than 10 years have found “success rates” of 90 percent or more following traditional THR.

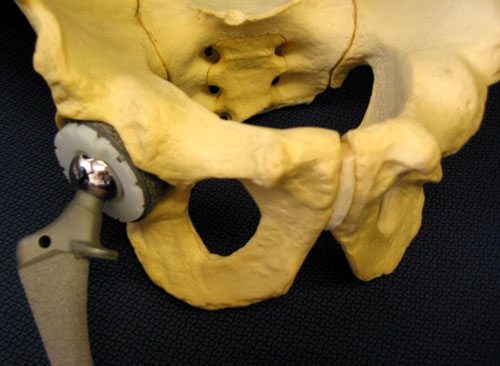
Distilled to its essentials THR involves surgically removing the arthritic parts of the joint (cartilage and bone) replacing the “ball and socket” part of the joint with artificial components made from metal alloys and placing high-performance bearing surface between the metal parts (see figures 1 and 2). Most commonly the bearing surface is made from a very durable polyethylene plastic but other materials (including ceramics newer plastics or metals) have been used. Patients typically spend a few days in the hospital after the procedure (3 to 5 days is most typical) and some patients benefit from a short inpatient stay in a rehabilitation facility after that to help transition back to living independently at home. Most patients will walk with a walker or crutches for 3 weeks and then use a cane for another 4 weeks; after that the large majority of patients are able to walk freely.
A bewildering number of different implant designs bearing surface materials and surgical approaches have been tried to achieve one seemingly straightforward goal: improving the quality of life for patients who have hip arthritis. As with any important life decision it makes good sense to get educated on those issues as they pertain to your hip.
The purpose of this article is to outline the essentials from a patient’s perspective: who should think about having THR done what questions should a prospective patient ask the doctor and why one surgical approach or type of THR implant might be good for one patient but not for another.
Not all surgical cases are the same, this is only an example to be used for patient education.
Symptoms & Diagnosis
Arthritis simply means “inflammation of a joint ” and itself is a very general term. Many of the more than 100 different conditions that cause joint inflammation also go on to cause permanent destruction of the weight-bearing surface of the hip which is called cartilage.
If you have ever eaten a drumstick you have seen cartilage: it is the white (or slightly yellow) smooth surface capping the end of the bone (see figures 3 and 4). The surface of normal human cartilage is much more slippery than a hockey puck sliding on ice.
In contrast arthritic cartilage may be cracked thinned or worn completely through to the bone. (see figures 5 and 6). If a doctor has told you that you have “bone-on-bone ” he or she means that the cartilage has completely worn away. Damaged cartilage (and certainly a bone-on-bone situation) does not glide well. As a result a severely arthritic joint may be stiff and it may feel like it grinds catches or locks with attempts at motion.
However the main symptom most people with hip arthritis have is pain. The pain typically is worse with activities or weight-bearing and is sometimes relieved by rest.
About 80 percent of patients with hip arthritis will have some pain in the groin or the front of the thigh; other typical pain patterns include pain in the back of the thigh the side of the thigh or the buttock. Sometimes with hip arthritis doesn’t cause hip pain at all because the symptoms show up as knee pain. Some patients with hip arthritis limp while walking sometimes with a “lurching” gait towards the arthritic side.
Although there are many types of arthritis (over 100 in fact) fewer than a handful of conditions account for over 95 percent of hip replacements performed. Some of these are:
- Osteoarthritis: Sometimes called degenerative joint disease (DJD) or “wear-and-tear” arthritis osteoarthritis is localized to the joint itself and does not have any systemic (whole body) manifestations. We know that most young patients (under age 50) with osteoarthritis of the hips have this condition as a result of one of several childhood hip conditions--but by the time the symptoms show up in adulthood the condition is treated as it would be for anybody with hip osteoarthritis.
- Post-traumatic arthritis: After a severe fracture of the pelvis or a dislocation of the hip the joint surface cartilage may suffer damage--either because of direct trauma or because of a loss of joint congruity (the good fit between the ball and the socket)--leading to pain and stiffness.
- Rheumatoid arthritis: This is a condition in which the body’s own cells attack joint surface cartilage. It may affect any joint in the body. The result of this is stiffness swelling and pain. The symptoms may vary over the course of the day and may wax and wane. There are many types of rheumatoid arthritis including some that affect children and young adults. Most patients with rheumatoid arthritis should be followed by a special kind of physician called a rheumatologist since there are so many new and successful medical therapies that can help control this disease. There are a large number of types of arthritis that are somewhat similar to rheumatoid arthritis; as a group these are called “inflammatory arthritis ” and they include conditions like systemic lupus erythematosis (SLE or lupus) psoriatic arthritis and others.
- Avascular necrosis (or osteonecrosis) of the Femoral Head: This is not exactly a type of arthritis but rather a condition in which the circulation to the “ball” of the “ball and socket” part of the hip joint becomes impaired. This causes the bone in a portion of the ball (called the femoral head) to die and collapse. The process can be quite painful. In addition the femoral head loses its round shape and flattens. Since the hip depends on a symmetric and congruent fit of the ball into the socket the resulting poor “fit” causes further stiffness and pain and leads to loss of the remaining joint surface cartilage (arthritis).
Avascular Necrosis (AVN), also known as osteonecrosis, isn't technically a form of arthritis, though it often leads to it. It occurs when the blood supply to the "ball" of the hip joint (the femoral head) is disrupted. Without adequate circulation, the bone tissue begins to die.
Avascular Necrosis (AVN), also known as osteonecrosis, isn't technically a form of arthritis, though it often leads to it. It occurs when the blood supply to the "ball" of the hip joint (the femoral head) is disrupted. Without adequate circulation, the bone tissue begins to die.
Many conditions cause pain in the area of the hip and most are not related to the hip joint at all. Some of these are:
- Spinal stenosis (or spinal arthritis): This condition commonly causes pain in the lower back that radiates to the buttocks (see figure 7). It may cause symptoms on both sides or just one. Many patients with this find that walking slightly stooped forward as with a shopping cart causes some relief of pain. Your orthopedic surgeon can easily tell this from hip arthritis with a good physical examination and some basic X-rays.
- Bursitis of the hip (greater trochanteric bursitis): Patients with this condition often have pain and tenderness over the “point” of the hip--the prominence on the outside of the thigh about 3 to 4 inches below the beltline (see figure 8). This condition may keep one from sleeping comfortably on that side. Bursitis is not in the hip joint at all but rather is an inflammation of a structure called a “bursa ” which is a fluid-filled sac between next to the femur (thigh bone) that helps tendons to glide smoothly over the bone. Again an orthopedic surgeon can readily distinguish this from hip arthritis with a good physical examination.
- Non-orthopedic conditions: Many diverse conditions can cause pain in the hips thighs or buttocks. Peripheral vascular disease (hardening of the arteries) can sometimes cause buttock or leg pain that is worse with activities or walking. Referred pain from intra-pelvic conditions in women (such as ovarian cysts) can cause pain in the groin and mimic hip joint symptoms as can inguinal (groin) hernias. A good family doctor can make sure none of these conditions are present using simple physical examination techniques.
According to the most recent statistics from the U.S. Centers for Disease Control and Prevention nearly 70 million Americans suffer from some form of arthritis or chronic joint symptoms.
Treatments
History and physical examination
An orthopedic surgeon will begin the evaluation with a thorough history and physical exam. Based on the results of these steps (s)he may order plain X-rays.
X-rays
If you have arthritis of the hip it will be evident on routine X-rays of the joint. X-rays taken with you standing up are more helpful than those taken with you lying down as the way your joint functions under load (i.e. standing) provides important clues about the severity of the arthritis to your physician.
Other tests
If your orthopedic surgeon suspects a problem with the hip joint but does not identify the source of the problem on plain X-rays (s)he may decide to order another test such as a Magnetic Resonance Imaging (MRI) study or a bone scan. These are more commonly ordered in the evaluation of conditions that are related to arthritis--such as avascular necrosis (osteonecrosis)--but are not always treated using the same techniques.
It is important to distinguish broadly between two types of arthritis: inflammatory arthritis (including rheumatoid arthritis, lupus and others) and non-inflammatory arthritis (such as osteoarthritis).
Although there is some level of inflammation present in all types of arthritis conditions that fall into the category of true inflammatory arthritis are often very well managed with a variety of medications and more treatments are coming out all the time. Individuals with rheumatoid arthritis and related conditions need to be evaluated and followed by a physician who specializes in those kinds of treatments called a rheumatologist. Excellent non-surgical treatments are available for these patients; those treatments can delay (or avoid) the need for surgery and also help prevent the disease from affecting other joints.
So-called non-inflammatory conditions including
Surgical options: bearing surfaces
Polyethylene metal or ceramic?
All hip replacements share one thing in common: they include a ball-and-socket joint. Which materials are used in the ball and in the socket--which together is called the “bearing ” like a bearing in a car--has the potential to affect the long-term durability of the joint replacement.
This is another area where technology may radically change the outcome of an operation; depending on how the research goes in this area hip replacement may look very different in 10 years than it does today. Or it may not.
Many bearing surfaces have been tried in the 40 or so years that hip replacements have been done. And many more have failed than succeeded. That is one reason to proceed with caution given that we now have a bearing surface (metal-on-polyethylene) that has a track record going back to the 1960s.
Polyethylene is a durable high-performance plastic resin. It is slippery (which is why it does well in a mobile joint like the hip) but it is known to wear out. In fact while more than 90% of metal-on-polyethylene bearing hip replacements (this is the most common bearing in use today) will be in service in 10 years many of those will not last 20 years. And when the plastic wears out it sometimes results in a destructive reaction causing bone loss around the joint. This can make repeat hip replacements (called revisions) more difficult.
Many types of plastics have been used in total hips but only one (ultra-high-molecular-weight polyethylene) has stood the test of time. Teflon (like the non-stick material used in frying pans) was tried and abandoned because of severe reactions by surrounding tissue. Other modifications of polyethylene have been tried (including carbon-reinforced plastic) and abandoned because of durability problems. In fact there is a new type of polyethylene gaining wide use today called highly-cross-linked polyethylene which shows promising results in the lab--but little if any data are available in people.
Ceramic bearing surfaces are sometimes used. These have been more popular in Europe than they have been in the United States. They may result in less aggressive wear but it is not known whether the wear they do cause will be more or less of a problem than wear from the traditional plastic bearings. Also fractures of ceramic bearings have been reported; as a result some of these bearings have been taken out of service at the direction of the FDA.
Finally, metal-on-metal bearings have become popular. Interestingly they were tried early on in the history of hip replacement but problems related to their manufacture led to surgeons moving on to other designs. Now those problems have been overcome and they offer the potential to reduce bearing wear to almost immeasurable amounts. Some scientists question whether these devices will lead to increased amounts of metal ions or corrosion products being released in the body but to date these concerns have not been proved to be serious. However because the renewed interest in these designs is fairly recent there is comparatively little follow-up published in scientific journals about the longevity of hip replacements using metal-on-metal bearing surfaces.
The choice of which bearing to use is still somewhat controversial and reasonable scientists surgeons and patients will sometimes disagree. This is one of the most exciting areas of research in the field of hip replacement surgery. But as with surgical approach it is worth considering the high likelihood of long-term success using traditional metal-on-polyethylene bearings when deciding whether to try another design that does not have results published beyond 10 years.
Surgical options: Hemi resurfacing hip arthroplasty
This is a technique that can be used for some patients with avascular necrosis (also called osteonecrosis) of the femoral head. As mentioned previously that is an arthritis-like condition of the hip; it may also affect the shoulders knees or ankles. It is caused by an interruption of the blood circulation to the ball (the femoral head) of the ball-and-socket hip joint. This may be caused by trauma to the hip excessive alcohol use use of medical steroids like prednisone or any of numerous disorders of blood clotting.
When avascular necrosis is allowed to run its course the result is usually severe degenerative joint disease and the treatment is usually traditional total hip replacement. Sometimes when the disease is caught early a joint-preserving procedure may be performed such as osteotomy (see below) core decompression or bone grafting.
In an intermediate stage of the disease avascular necrosis affects only the ball and not the socket; sometimes the top of the ball collapses resulting in a loss of roundness and this causes pain. At this stage a resurfacing hip replacement may be an option. This involves putting a round metal “cap” on the ball and keeping the patient’s own socket.
Advantages of this include the fact that it does not take away much bone (perhaps leaving more options available for subsequent reoperations) and that it is reasonably durable. Two studies have found that between 60% and 70% of these devices remain in service 10 years after the surgery. This doesn’t sound great compared to total hip replacement which has more than 90% success at that same time period but one must remember that patients with this stage of avascular necrosis are often quite young--anywhere from their 20s to 40 or so--and so total hip replacement is not considered an ideal approach for them.
The main disadvantage to this procedure apart from the failure rate is that pain relief is somewhat less than with traditional total hip replacement--perhaps 80% as good--so many of these patients are left with some discomfort even after the surgery although most patients feel much better with the hemi resurfacing arthroplasty than they did before.
Patients with avascular necrosis have a complex set of choices to make and so it is best for them to find a surgeon who is extremely comfortable and experienced with a wide array of options to treat the painful hip.
Surgical options: Pelvic osteotomy and hip fusion
About osteotomy and hip fusion
Osteotomy is a procedure in which the bone around the socket of the hip joint is surgically cut so that the socket itself can be re-oriented. This is best suited for young people with relatively early stages of arthritis particularly if the arthritis was caused by a childhood hip condition called developmental dysplasia of the hip.
Hip fusion is an operation that was more popular in the days before hip replacements were widely performed. This consists of surgically attaching the femur (thigh bone) to the pelvis and causing the two bones to heal together to become one. It results in loss of motion at the hip joint which is obviously a disadvantage but it is very reliable at relieving pain. It is seldom done anymore because most patients prefer to maintain motion about the hip but in the right circumstances it can still be a good choice. Patients who are otherwise poor candidates for hip replacement--such as young people who plan to continue doing heavy manual laborer for a living or young patients with prior hip joint infections--may decide that hip fusion is right for them.
Effectiveness
Current evidence suggests that traditional total hip replacements last more than 10 years in more than 90% of patients. More than 90% of patients report having either no pain or pain that is manageable with use of occasional over-the-counter medications. The large majority of hip replacement patients are able to walk unassisted (i.e. without use of a cane) without any limp for reasonably long distances. Many have no distance restrictions at all and resume hiking golfing bicycling and other non-impact recreational activities (see figure 9).
As mentioned there are no studies to date documenting the short-term or long-term effectiveness of minimally-invasive hip replacement and there are no studies that have proved that the joint replacement components can be reliably inserted with equal success or safety through the smaller incision used in minimally-invasive hip replacement techniques.
In the event that a total hip replacement requires re-operation sometime in the future the results are generally good--although often not as good as one typically gets with an uncomplicated first-time hip replacement. The results of repeat hip replacements (called “revisions”) often depend on a number of factors that are not in the surgeon’s (or the patient’s) control such as: infection bone loss and condition of the muscles and other soft tissues around the hip joint. But in general revision hip replacement can achieve a durable result and provide substantial relief of pain.
There is good evidence that the experience of the surgeon correlates with outcome in all kinds of joint replacements including total hip replacements. It is important that the surgeon performing the technique be not just a good general orthopedic surgeon but an expert experienced total hip replacement surgeon as well. It is reasonable to ask a surgeon whether (s)he concentrates his/her practice on joint replacements or whether (s)he does all kinds of orthopedic surgery.
Urgency
Total hip replacement for arthritis is elective surgery. With few exceptions it does not need to be done urgently and can be scheduled around your other important life events.
Risks
Like any major surgical procedure total hip replacement is associated with certain medical and surgical risks. Although major complications are uncommon they may occur. The possibilities include infection blood clots bleeding or blood transfusion and anesthesia-related or medical risks. Certain hip-specific risks like infection at the surgical site (typically less than 1.5%) dislocation (where the ball comes out of joint; less than 1% with one popular surgical technique) or other problems may also occur. However the overall frequency of major complications following total hip replacement is low typically less than 5 percent (one in 20) depending on the individual’s medical risk factors.
Later risks include the possibility that the device may loosen from the bone; late infections and dislocations may also occur. But again numerous studies have shown that a technically well-performed total hip replacement is more than 90 percent likely to be in service and functioning well more than 10 years after the surgery.
Managing risk
Most of the major risks of total hip replacement can be treated. The best treatment though is prevention. At the UW orthopedic surgeons will use antibiotics before during and after surgery to minimize the likelihood of infection. They will take steps to decrease the likelihood of blood clots such as early patient mobilization and use of blood-thinning medications in some patients. Patients are evaluated by a good internist and/or anesthesiologist in advance of the surgery in order to decrease the likelihood of a medical or anesthesia-related complication. Great care is taken to be certain that the technical elements of the operation that are so important to success are correctly performed.
Again the overall likelihood of a severe complication is generally less than 5 percent when such steps are taken.
Preparation
Patients undergoing a total hip replacement performed at the University of Washington Medical Center usually will undergo a pre-operative surgical risk assessment. When necessary further evaluation will be performed by an internal medicine physician who specializes in pre-operative evaluation and risk-factor modification. Some patients will also be evaluated by an anesthesiologist in advance of the surgery.
Routine blood tests are performed on all pre-operative patients; chest X-rays and electrocardiograms are obtained in patients who meet certain age and health criteria as well.
At the University of Washington surgeons will spend time with the patient in advance of the surgery making certain that all the patient's questions and concerns as well as those of the family are answered.
Timing
Total hip replacement for arthritis is elective surgery. With few exceptions it does not need to be done urgently and can be scheduled around your other important life events.
Costs
The surgeon's office should provide a reasonable estimate of:
- the surgeon's fee
- the hospital fee and
- the degree to which these should be covered by the patient's insurance.
Surgical team
Total hip replacement requires an experienced orthopedic surgeon and the resources of a large medical center. Patients have complex medical needs and around surgery often require immediate access to a multiple medical and surgical specialties and in-house medical physical therapy and social support services.
Finding an experienced surgeon
There is good evidence that the experience of the surgeon performing total hip replacement affects the outcome. It is important that your surgeon not only be an experienced orthopedic surgeon; (s)he also should have a high level of skill and experience with total hip replacements.
Some questions to consider asking your knee surgeon:
- Are you board-certified in orthopedic surgery?
- Have you done a fellowship (a year of additional training beyond the five years required to become an orthopedic surgeon) in joint replacement surgery?
- Does your practice focus on joint replacement surgery and the problems of joint replacement patients?
Facilities
A large hospital usually with academic affiliation and equipped with state of the art radiologic imaging equipment and intensive medicine care unit is clearly preferable in the care of patients with hip arthritis.
Technical details
Because there are now so many techniques that are used to perform total hip replacements and because the issues pertaining to those techniques have been reviewed earlier in this article (need t link to prior sections) this section will summarize the “basics” of traditional total hip replacement.
Any of several techniques for anesthesia are possible: general (going to sleep) spinal or epidural. After anesthesia has been successfully achieved total hip replacement surgery begins by performing a sterile preparation of the skin over the hip to prevent infection.
Next a well-positioned incision is made down the side of the hip. As already discussed the location and length of the incision varies widely by approach and based on the patient’s own anatomy.
Deeper tissues (muscles and tendons) are either spread or incised and prepared for later repair. The hip capsule (a thick covering directly on top of the ball and socket joint) is then opened. The ball is gently levered out of the socket and the arthritic ball is removed using a saw.
At this point the damaged arthritic cartilage on the socket is removed using a scraping tool called a reamer and the socket (which may be misshapen from arthritis) is shaped to form a hemisphere. An artificial socket (called the acetabular component) is now inserted usually without using bone cement. Sometimes additional screws are used to hold the component firmly to the bone during the critical weeks following surgery when the patient’s bone will attach itself to the metal on the artificial socket.
Next the inside of the thigh bone (femur) is prepared using motorized and hand-held tools to shape it to accept a stem at one end of which is the new artificial ball called the femoral head. Once the stem is inserted leg length and joint stability are verified and the final components are inserted.
The tissues are cleaned with sterile saline solution (liquid) any deep tissues that were incised are now repaired and the skin is closed. A surgical drain may be used at the surgeon’s discretion.
Anesthetic
As mentioned total hip replacement may be performed under epidural spinal or general anesthesia. The choice is made in consultation with the surgeon and anesthesia provider.
Length of total hip arthroplasty hip resurfacing and minimally-invasive hip surgery
No two hip replacements are alike and there is some variability in operative times but the range is typically between one and two hours of actual operative time.
Pain and pain management
There are several options for pain control. Most commonly a patient will have control over his/her own pain management using a Patient-Controlled Anesthesia (PCA) device. Using an electronic device programmed with a safe but effective dosing approach the patient uses a button to tell the machine when to administer a dose of painkiller either through an intra-venous (I.V.) tube in the arm or through the epidural catheter in the lower back if one was used.
Use of medications
Following discharge from the hospital most patients will take pain pills (usually Percocet, Vicodin or Tylenol #3) for an average of two to six weeks after the procedure mainly to help with physical therapy and home exercises for the hip. Some patients don’t even need the medications for that long.
Effectiveness of medications
Most patients report that although there is some post-operative pain it is quite manageable with the PCA device. Most patients also report that the pain steadily declines with each passing day.
Hospital stay
The average hospital stay is three days in length after a total hip replacement.
Recovery and rehabilitation in the hospital
Physical therapy is started on the day of (or the day after) surgery. Patients generally are encouraged to walk and to bear as much weight on the leg as they are comfortable doing. Other exercises to help with balance and getting into and out of bed are initiated on the day of surgery or the next morning.
At the UW Medical Center The physical therapist is an integral member of the “team” approach and the patient’s own high level of motivation and enthusiasm for recovery are very important elements in determining the ultimate outcome.
Hospital discharge
Patients are encouraged to walk using a walker crutches or cane as needed. Immediate weight bearing is permitted in most cases depending on other surgical circumstances.
Patients are allowed to shower following hospital discharge provided that there is no drainage coming from the incision site. We do not recommend that patients drive while taking narcotic-based pain medications; on average patients are able to drive between two and four weeks after the surgery.
Each patient will be instructed in “Hip Precautions” after surgery. This is a short list of restrictions on particular motions designed to prevent dislocation of the joint replacement. Which specific precautions are used in an individual case depends on the approach used but in general patients are encouraged to avoid the extremes of hip rotation (twisting motions of the leg) and flexion (bending forward). Low chairs low couches and swivel chairs should be avoided. After about six weeks some of those restrictions are relaxed--for example most patients can easily put on shoes and socks once they’ve recovered from surgery and the surgeon gives them the OK--but others including extreme flexion and rotation should always be limited to be on the safe side.
Convalescent assistance
Patients who live alone or who feel they would benefit from the extra support or attention usually are able to go to an inpatient rehabilitation hospital or an extended-care facility after hospital discharge. At UW that rehab hospital is on-site so the switch to rehab doesn’t even require going in a car or ambulance.
Sometimes younger patients or patients who have enough help at home will decide to go straight home after hospital discharge.
Physical therapy
Following hospital discharge (or discharge from inpatient rehabilitation) patients who undergo total hip replacement will participate in either home physical therapy or outpatient physical therapy to a location close to home.
Depending on the surgical approach used that therapy can begin right after discharge or it will start at six weeks after the surgery (the time when tissue healing of an important tendon has taken place). The surgeon will help you make the necessary arrangements.
The length of physical therapy varies based on patient age fitness and level of motivation but usually lasts about a month. Two to three therapy sessions per week are average for this procedure.
The specific therapy procedures vary with surgical approach but balance safe walking and reviewing hip precautions are emphasized early and muscle strengthening are goals later on.
Can rehabilitation be done at home?
As mentioned this depends on each patient’s individual circumstances. Age fitness level and having adequate help around the house are some of the elements that guide the choice.
All patients are given a set of home exercises to do between supervised physical therapy sessions and the home exercises make up an important part of the recovery process. However supervised therapy--which is best done in an outpatient physical therapy studio--is extremely helpful and those patients who are able to attend outpatient therapy at the appropriate times after hospital discharge are encouraged to do so.
For patients who are unable to attend outpatient physical therapy home physical therapy is arranged.
Usual response
On average patients walk with a walker (or two crutches) for about 3 weeks then a cane for another month or so.
The deep pain from the arthritis is usually noticeably absent right after surgery; the post-operative pain gradually improves and most patients have quit taking narcotic pain tablets by about a month after surgery.
The large majority of patients are able to walk without a limp and to resume reasonable personal and recreational activities gradually in the weeks and months following surgery.
Returning to ordinary daily activities
The goal of total hip replacement is to return patients to a good level of function without hip pain. The large majority of patients are able to achieve this goal. However since the joint replacement components have no capacity to heal damage from injury sustained after surgery we offer some common-sense guidelines for athletic leisure and workplace activities:
Recommended:
- Swimming
- Water aerobics
- Cross-country skiing or Nordic Track
- Cycling or stationary bike (see figure 10)
- Golf
- Dancing
- Sedentary occupations (desk work)
Permitted:
- Hiking
- Gentle doubles tennis
- Light labor (Jobs that involve driving walking or standing but not heavy lifting)
Not recommended:
- Jogging/running
- Impact exercises
- Sports that require twisting/pivoting (aggressive tennis basketball racquetball)
- Contact sports
- Heavy labor
Since the joint replacement includes a bearing surface which potentially can wear walking or running for fitness are not recommended. Patients generally feel well enough to do this and so need to exercise judgement in order to prolong the life-span of the implant materials. Swimming water exercises cycling and cross country skiing (and machines simulating it like Nordic Track) can provide a high level of cardiovascular and muscular fitness without excessive wear on the prosthetic joint materials (see figure 10).
As mentioned certain precautions should be maintained for life in order to minimize the likelihood of dislocating the ball from the socket. Avoiding extreme twisting and bending from the hip are the most important of these.
Costs
Most insurance plans cover the costs of total hip replacement (including anesthesia surgical fees hospital stay lab tests and medications). Many also approve inpatient rehabilitation following the surgery. Most cover home or outpatient physical therapy following hospital discharge.
Many insurance plans have deductibles or co-payments; the only way to be sure in each individual’s case is to contact your insurance provider. UW has expert social workers who can help guide patients through the process.
Medicare pays 80% of the costs and good Medicare supplemental programs usually cover the balance. Again the only way to know what your supplemental covers is to ask. UW social workers can help with this as well.
Summary of total hip arthroplasty hip resurfacing and minimally-invasive hip surgery for hip arthritis
Total hip replacement is a reliable operation in which the arthritic portions of a hip joint can be replaced with an artificial bearing surface. Pain is substantially improved and function regained in more than 90% of patients who have the operation.
Like any major procedure there are risks to total hip surgery and the decision to have a hip replacement must be considered a quality-of-life choice that individual patients make with a good understanding of what those risks are.
Hip replacement is a surgical technique that has many variables; like most areas of medicine ongoing research will continue to help the technique evolve. It is important to learn as much as possible about the condition and the treatment options that are available before deciding whether – or how – to have a hip replacement done. While many of the changes now being explored in the field of total hip replacement may eventually be shown to be legitimate advances – perhaps including so-called minimally-invasive surgical techniques as well as alternative bearing surfaces – it is important to compare them carefully to traditional total hip replacement performed using well established techniques which we know are 90-95% likely to provide pain relief and good function for more than 10 years after the surgery.