 Edited By Daphne M. Beingessner, M.D., Associate Professor, UW Orthopaedics & Sports Medicine
Edited By Daphne M. Beingessner, M.D., Associate Professor, UW Orthopaedics & Sports Medicine
Last updated: January 29, 2010
Overview
The elbow is the second most commonly dislocated major joint. Elbow dislocations frequently occur due to trauma such as falls from heights or motor vehicle collisions. Elbow dislocations can be either simple or complex. Higher energy elbow dislocations are often associated with fractures of various parts of the elbow. These higher energy injuries are defined as “complex” elbow dislocations. An elbow dislocation is defined as “simple” if there is no associated fracture. Simple dislocations typically do not require surgery. However when a fracture has occurred, the elbow may remain unstable if surgery is not performed. The goal of treatment in both types of injury is to restore a functional range of motion and a pain-free joint for the patient.
Characteristics of elbow dislocations
The elbow is an inherently stable joint. Dislocation usually occurs as a result of a significant event such as a fall or car accident. Patients with dislocated elbows usually experience considerable pain, obvious deformity and swelling. They may also experience numbness or tingling in their hand after injury.
Types
The two general types of elbow dislocation are:
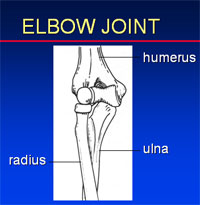
- Simple elbow dislocation: The radius and ulna articulate with the humerus at the elbow. When the radius and ulna become dissociated from the humerus without associated fracture, this injury is called a simple dislocation. Typically the radius and ulna move behind the humerus.
- Complex elbow dislocation: This injury is a simple dislocation combined with a fracture of the humerus, radius, ulna or a combination of all three bones.
Similar conditions
Small elbow fractures associated with dislocations can be missed on x-rays (radiographs) so the images must be carefully reviewed. The diagnosis of any associated fractures is important in deciding the appropriate management of the injury.
Incidence and risk factors
The elbow is the second most common major joint (after the shoulder) to experience dislocation.
Diagnosis
The clinician must obtain a complete patient history and information about the accident, including time of injury mechanism and associated injuries. Next the entire upper extremity is examined. The skin is inspected for swelling, bruising, open wounds and obvious deformity. The joint is then examined by feeling and pressing (palpitating) for tenderness. A detailed examination of the nerves (median radial ulnar) crossing the elbow must be done. An assessment of the vascular status of the arm is mandatory. Plain radiographs are then performed to define the injury.
Exercises
Exercises are the mainstay of treatment after reduction and/or surgery for elbow dislocations and/or fracture-dislocations. Rehabilitation is essential in either the surgical or non-surgical treatment of elbow fracture-dislocations. After closed reduction, exercises to improve range of motion must be performed. After surgery, exercise is an essential part of rehabilitation and a key component of a successful treatment outcome.
Possible benefits of elbow surgery
Simple elbow dislocations are associated with damage to the ligaments around the elbow. Typically these dislocations heal uneventfully without surgery. However, in rare instances if the elbow remains unstable (i.e. re-dislocates partially or completely) surgery may be required.
Complex dislocations often remain unstable following closed reduction. In these cases, surgery to repair the fractures and ligaments is often required to restore stability to the joint.
Types of surgery recommended
The surgery performed depends on what area is fractured. Typical patterns include the following:
- If the radial head (top end of the radius) is fractured, it can be repaired with small screws with or without plates. If the fracture is not repairable, the radial head is replaced with a metallic implant.
- If the coronoid (top of the ulna in the front of the joint) is fractured, it can be repaired with screws or sutures.
During these procedures, the ligaments on the lateral part (outside) of the elbow are repaired. Occasionally, the elbow still remains unstable at this point and the surgeon will have to repair the medial (inner) ligaments and even more rarely will have to apply a hinged external fixator (pins and bars outside the skin) to provide the necessary joint stability while the soft tissues heal. This latter procedure is rarely needed.
Who should consider elbow surgery?
Patients with residual instability following closed reduction of a simple dislocation, although rare, will require surgery. Patients with significant fractures almost always require surgery.
What happens without surgery?
In general if an elbow remains partially or completely dislocated, the patient will experience considerable pain, stiffness, decreased function and eventually arthritis.
Surgical options
The surgery performed depends on what parts of the elbow are fractured. Typical patterns include the following:
1. If the radial head (top end of the radius) is fractured, it can be repaired with small screws either with or without plates. If the fracture is not repairable, the radial head is replaced with a metallic implant.
2. If the coronoid (top of the ulna in the front of the joint) is fractured, it can be repaired with screws or sutures.
During these procedures, the ligaments on the lateral part (outside) of the elbow are repaired. Occasionally, the elbow still remains unstable at this point and the surgeon will have to repair the medial (inner) ligaments and even more rarely will have to apply a hinged external fixator (pins and bars outside the skin) to provide the necessary joint stability. This latter procedure is rarely needed.
Effectiveness
Typically simple elbow dislocations heal without surgery.
Historically, complex elbow injuries had poor outcomes. However, with standard treatment protocols and a better understanding of the injury patterns, outcomes have significantly improved. Although patients may not regain a full range of motion, patients can expect to regain a functional range of motion in their injured elbow. One of the most common complications of any elbow injury is stiffness. This problem may occur in both simple and complex injuries. However, with restoration of stability range of motion, exercises can be started early decreasing the risk of residual pain and stiffness.
Urgency
For simple elbow dislocations, the elbow should be reduced as soon as possible. This is accomplished with adequate sedation and gentle traction along with manual realignment of the joint.
Complex elbow dislocations should also undergo closed reduction as soon as possible to realign the joint as best as possible. If surgery is deemed necessary, it should be performed within the first week following injury before significant scarring and stiffness occurs. This enables the surgeon to see the injury more clearly during surgery.
Risks
As with any operation, there is risk of infection, possible damage to nerves or blood vessels in the surrounding tissue. Despite surgery there is also a risk of the elbow remaining unstable or fractures not healing, although this is not common. There is also risk of stiffness from scar tissue formation or from extra bone formation within the soft tissues. Patients should be aware that their elbow will not be like their other “normal elbow” but rather the goal is to provide a functional pain-free range of motion for daily activities.
Managing risk
All risks in elbow fracture-dislocation surgery do not commonly occur, however the most common is continued elbow stiffness. If this occurs, further surgery including scar and bone removal may be required to adequately restore a functional pain-free range of motion for daily activities.
Timing
For simple elbow dislocations, the elbow should be reduced as soon as possible. This is accomplished with adequate sedation and gentle traction along with manual realignment of the joint.
Complex elbow dislocations should also undergo closed reduction as soon as possible to realign the joint as best as possible. If surgery is deemed necessary, it should be performed within the first week following injury before significant scarring and stiffness occurs. This enables the surgeon to see the injury more clearly during surgery.
Costs
The surgeon’s office should provide a reasonable estimate of:
- The surgeon’s fee
- The hospital fee and
- The degree to which these should be covered by the patient’s insurance.
Surgical team
Elbow fracture-dislocation surgery is technically demanding. There are relatively few surgeons who have extensive experience performing the procedure. Patients should inquire as to the number of elbow surgeries the surgeon performs each year and the number performed at the medical center each year.
Finding an experienced surgeon
Surgeons specializing in elbow fracture-dislocation surgery can be located through university medical schools, county medical societies or other state orthopedic societies.
Facilities
Elbow fracture-dislocation surgery is usually performed in medical centers where they are done regularly and have teams and facilities specially designed for this type of surgery. These teams include nurses and therapists who are accustomed to assisting patients in their recovery.
Anesthetic
Elbow fracture-dislocation surgery is usually performed under general anesthesia. The patient may wish to discuss his or her preferences with the anesthesiologist before surgery.
Length of elbow surgery
The length of surgery varies depending on the case. It usually takes two to five hours. In addition, several hours will be needed for preoperative preparation (two hours) and postoperative recovery (two to four hours).
Pain and pain management
Typically patients are admitted to the hospital for three days. They usually experience considerable pain after surgery for the first 24 to 48 hours.
During this time, they will receive narcotic analgesics. Narcotics (such as morphine or Demerol) are usually necessary for three days following surgery and are given by injection. Thereafter pain is controlled with oral medications such as Hydrocodone or Tylenol with codeine.
Use of medications
Initially following surgery, pain medication is usually administered in the hospital intravenously or intramuscularly. Sometimes patient controlled analgesia (PCA) is used to allow the patient to administer the medication as needed. Oral medications are started in the hospital and continued once the patient goes home. They are usually only needed for the first two weeks after the procedure.
Effectiveness of medications
Pain medications can be very powerful and effective. Their proper use lies in the balancing of their pain relieving effect and other less desirable effects. Good pain control is an important part of postoperative management.
Important side effects
Pain medications can cause drowsiness, slowness of breathing, difficulties in emptying the bladder and bowel, nausea, vomiting and allergic reactions. Patients who have taken substantial narcotic medications in the recent past may find that usual doses of pain medication are less effective. For some patients balancing the benefits and the side effects of pain medication is challenging. Patients should notify their surgeon if they have had previous difficulties with pain medications or pain control.
Hospital stay
After elbow fracture-dislocation surgery, the patient spends an hour or so in the recovery room. A drainage tube is usually used to remove excess fluid from the surgical area. The drain is in place for several days. Bandages cover the incision. They are changed on the second or third day after surgery and the patient is started on range of motion exercises with the physical therapist while in hospital. Patients are discharged after they are comfortable and can demonstrate they can perform the range of motion exercises properly.
While in the hospital, the patient wears a removable splint. He or she takes off the splint for exercise. When not exercising, the patient should wear the splint for added comfort and protection.
Recovery and rehabilitation in the hospital
Typically the patient cannot perform any heavy lifting activities for at least six weeks following surgery. During the first six weeks to three months, the primary focus is on regaining motion. Following fracture healing and restoration of a functional range of motion, strengthening and work-hardening (or preparing the elbow for work activities). exercises are begun. Patients may need to be off work for four to six months or longer depending on the injury and their job requirements.
Hospital discharge
The patients are instructed in proper follow-up care and physical therapy appointments are scheduled.
Convalescent assistance
The patient’s need for convalescent assistance after fracture-dislocation surgery depends on the severity of the injury. If the dominant arm is injured, there are other injuries present, and the patient lives alone or is elderly, they may require convalescent care during recovery.
Physical therapy
Typically, the patient cannot perform any heavy lifting activities for at least six weeks following surgery. During the first six weeks to three months, the primary focus is on regaining motion. Following fracture healing and restoration of a functional range of motion, strengthening and work-hardening or preparing for work exercises are begun. Patients may need to be off work for four to six months or longer depending on the injury and their job requirements.
Rehabilitation options
After elbow fracture-dislocation surgery, patients typically require the assistance of a therapist at least two to three times per week. However exercises need to be performed at home at least three to four times per day. Splinting to improve flexing or extension may be required.
Can rehabilitation be done at home?
Exercises after elbow fracture-dislocation surgery need to be performed at home at least three to four times per day. Splinting to improve flexing or extension may be required.
Usual response
Following elbow fracture-dislocation surgery, patients typically regain a functional range of motion within the first six to eight weeks.
Risks
The biggest risk is not performing post-operative rehabilitation. By not complying with their prescribed exercise program and recovery guidelines, patients will reduce the likelihood of a successful outcome.
Duration of rehabilitation
Following elbow fracture-dislocation surgery, typically three to six months of therapy is required.
Returning to ordinary daily activities
The length of time it takes to return to daily activities after elbow fracture-dislocation surgery depends on the injury severity and whether or not the injury affected the patient’s dominant arm.
Long-term patient limitations
After full recovery from elbow fracture-dislocation surgery, there are no limitations on the patient.
Costs
The surgeon and therapist should provide information on the usual cost of rehabilitation. The program is usually cost effective as it is based predominately on home exercises.
Summary of elbow surgery for elbow dislocations.
- Elbow dislocations can be simple or complex.
- Surgery may be required to restore elbow stability and to facilitate early range of motion.
- Stiffness may occur with or without surgery.
- There are many surgical options depending on the injury pattern. Therefore, an experienced surgeon should perform this type of surgery.
- Physical therapy in the form of range of motion exercises is the most essential part of the post-operative rehabilitation.